(20) The Hot Quadrate Sign: A Radiologic Hallmark of SVC Syndrome
Saturday, October 18, 2025
6:00 PM - 7:30 PM East Coast USA Time
Grant Zydeck, B.S – Medical Student, Wayne State School of Medicine; Priya Gupta, M.D – Radiology Resident, Henry Ford Hospital; Mitchell Giordano, M.D – Interventional Radiologist, Henry Ford Hospital
Purpose: The purpose of this case-based educational exhibit is to explore the radiologic basis, clinical context, and significance of the hot quadrate sign.
Material and Methods: We present a case of a 54-year-old female with no significant known prior medical history who presented with worsening facial swelling and right greater than left bilateral upper extremity swelling. A contrast-enhanced CT of the abdomen and pelvis demonstrated a large anterior mediastinal mass resulting in narrowing of the superior vena cava (SVC) with tumor thrombus extending into the SVC and bilateral upper extremity deep veins. Pathology of the biopsied mediastinal mass revealed poorly differentiated non-small cell carcinoma.
Results: Review of the initial CT abdomen and pelvis revealed findings highly suspicious for SVC syndrome. The medial aspect of segment IVb, also called the quadrate lobe, demonstrated geographic, focal hyperperfusion compatible with the hot quadrate sign. This results from venous obstruction and altered hepatic perfusion and is most commonly associated with type IV SVC obstruction. This subtype is characterized by concomitant SVC and azygos venous obstruction, which leads to rerouting of venous blood through anterolateral thoracoabdominal collaterals that ultimately drain into the left branch of the portal vein supplying the quadrate lobe. On arterial phase CT, this results in a focal wedge shaped hyperenhancement ultimately favoring a hepatic pseudolesion secondary to SVC obstruction.
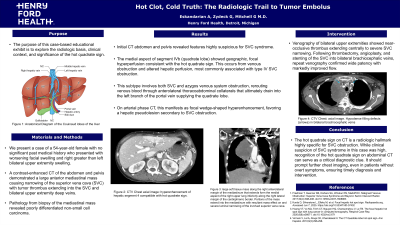
Initial venography of bilateral upper extremities demonstrated near occlusive thrombus starting from the proximal brachial vein on the right and from the proximal brachiocephalic vein on the left extending centrally to an area of severe narrowing of the SVC. After completion of thrombectomy, angioplasty, and stenting of the SVC into bilateral brachiocephalic veins, venography showed wide patency of the stents with markedly improved flow through the previously occluded vessels.
Conclusions: The hot quadrate sign on CT is a radiologic hallmark highly specific for SVC obstruction. While clinical suspicion of SVC syndrome in the index case was relatively high, the presence of a hot quadrate sign on contrast-enhanced abdominal CT can serve as an important clue to prompt further evaluation with cross-sectional chest imaging, particularly in patients without overt symptoms, ensuring that appropriate intervention is pursued when clinically warranted.