(88) A Retrospective Review of Balloon Dissection During Thermal Ablation in Renal and Liver Tumors
Saturday, October 18, 2025
6:00 PM - 7:30 PM East Coast USA Time
Ripal Gandhi, M.D. – Physician, Miami Cardiac and Vascular Institute; Gina Landinez, M.D. – Physician, Miami Cardiac and Vascular Institute; Govindarajan Narayanan, M.D. – Physician, Miami Cardiac and Vascular Institute; Constantino Pena, M.D. – Physician, Miami Cardiac and Vascular Institute; Brian Schiro, M.D. – Physician, Miami Cardiac and Vascular Institute; Nathan Gilmore, B.S. – Medical Student, Miami Cardiac and Vascular Institute; Elizabeth Ruiz, B.S. – Student, Miami Cardiac and Vascular Institute; Bente Van Den Bemb, M.D. – Physician, Miami Cardiac and Vascular Institute
Purpose: To evaluate the technical feasibility, safety, and early oncologic efficacy of CT‑guided balloon dissection used as an adjunct to percutaneous cryoablation or microwave ablation for renal and hepatic tumors.
Material and Methods: This IRB-approved, STROBE-compliant retrospective study reviewed patients who underwent CT-guided percutaneous cryoablation or microwave ablation (MWA) with balloon dissection used to separate tumors from adjacent bowel. Eligible patients had follow-up imaging and were fit for general anesthesia. Balloon placement was performed using a Yueh needle and Benton wire, followed by inflation of Atlas or Conquest balloons to displace adjacent structures. Ablations were conducted using standard cryoablation systems or the Emprint HP™ MWA platform. Technical success required ≥5 mm post-ablation margin; safety was assessed per CTCAE v5. Descriptive statistics were used for analysis.
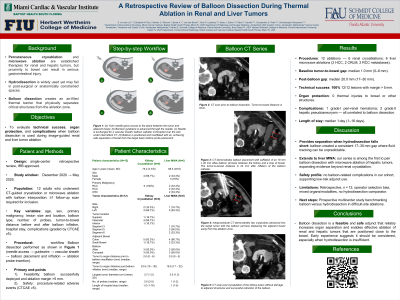
Results: Eight patients (4 cryoablation, 4 microwave ablation) underwent CT-guided thermal ablation with balloon dissection between tumor and bowel. Median tumor-to-bowel distance increased from 0.5 mm to 21.2 mm after balloon inflation. Technical success (complete ablation with ≥5 mm margin) was achieved in all cases. No thermal injuries to adjacent structures occurred. One cryoablation patient experienced a self-limited hematoma; one MWA patient had a pseudoaneurysm that was successfully embolized. No complications were directly related to balloon placement.
Conclusions: Balloon dissection proved to be a safe and effective adjunctive method for displacing bowel during renal and hepatic tumor ablations, offering reliable separation even in anatomically complex cases. Compared to hydrodissection, balloon use may offer better control in limited or post-surgical spaces. Prior studies in renal cryoablation and hepatic RFA support its efficacy, but data remain limited in the setting of MWA. This study adds to emerging evidence that balloon dissection may expand ablation eligibility for tumors near critical structures, though broader studies are needed to confirm long-term outcomes and comparative efficacy.