(3) Bridging and Downstaging in HCC: Role of TACE vs TARE in Transplant Eligibility
Saturday, October 18, 2025
6:00 PM - 7:30 PM East Coast USA Time
Jad Elharake, MPH – Medical Student, The Ohio State University College of Medicine; Elliott Fite, MS – Medical Student, The Ohio State University College of Medicine; Mina Makary, MD – Associate Clinical Professor of Radiology, Department of Radiology, The Ohio State University Medical Center
Purpose: Transarterial chemoembolization (TACE) and transarterial radioembolization (TARE) can be used as a bridge to transplantation in patients with hepatocellular carcinoma (HCC) who are initially ineligible for liver transplant (LT) due to tumor size, number, or location. This abstract explores the comparative indications and outcomes of both TACE and TARE in bridging and downstaging HCC for transplant eligibility.
Material and Methods: A systematic review of PubMed literature was conducted. Data on patient selection, HCC characteristics, and oncological outcomes of TARE and TACE for downstaging or bridging in LT were analyzed. Eligibility for screening required studies to focus on TARE or TACE as the primary locoregional therapy for downstaging or bridging in LT, involving human participants, and providing sufficient experimental design details.
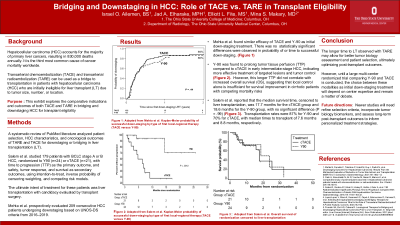
Results: A multiregional study involving 7 centers and 4 united networks of organ sharing (UNOS) regions compared TACE (n = 132) and TARE (n = 62) as initial downstaging treatments. No differences were found in response, probability, time to successful downstaging, waiting list dropout, or LT [1]. Despite the comparable efficacy of TACE and TARE in downstaging HCC, TARE is associated with a longer time to LT (6.5 months vs. 4.8 months, p=0.02) [2]. Another study corroborated these findings, noting a longer time to LT in the TARE group, along with better tumor control and fewer complications. TARE patients had a transplantation rate of 87%, compared to 70% in the TACE group [3]. Additionally, a RCT reported a higher tumor response and downstaging rate for LT with TARE (9/32) compared to TACE (4/34) (95% CI: 0.14, 0.60; P < .001) [4]. Overall, TARE is likely to be used preferentially in those with infiltrative tumors, portal vein invasion, larger tumors (>2 segments) and those with progression of tumor despite use of TACE [5].
Conclusions: TACE and TARE are both valuable modalities for bridging and downstaging HCC, with TARE demonstrating increasing efficacy, especially for large (>2 segments) and infiltrative tumors. The longer time to LT observed with TARE may allow for better tumor biology assessment and patient selection, ultimately optimizing post-transplant outcomes. Future studies are needed to refine selection criteria, incorporate tumor biology biomarkers, and assess long-term post-transplant outcomes to inform personalized treatment strategies.