(50) Updates in Transarterial Chemoembolization in Neuroendocrine Liver Metastases
Saturday, October 18, 2025
6:00 PM - 7:30 PM East Coast USA Time
John Heyniger, BS – Medical Student, The Ohio State University College of Medicine; Mina Makary, MD – Interventional and Diagnostic Radiologist, The Ohio State University Wexner Medical Center
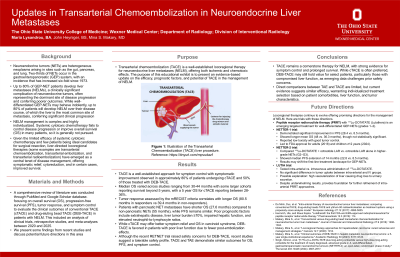
Purpose: Transarterial chemoembolization (TACE) is a well-established locoregional therapy for neuroendocrine liver metastases (NELM), offering both ischemic and chemotoxic effects. The purpose of this educational exhibit is to present an evidence-based update on the efficacy, prognostic factors, and potential of TACE in the management of NELM.
Material and Methods: A comprehensive review of literature was conducted using PubMed and Google Scholar databases focusing on overall survival (OS), progression-free survival (PFS), tumor response, and symptom control to evaluate the clinical outcomes of conventional TACE (cTACE) and drug-eluting bead TACE (DEB-TACE) in patients with NELM. This included an analysis of clinical trials, retrospective studies, and meta-analyses between 2020 and 2025.
Results: TACE is a well-established approach for symptom control with symptomatic improvement observed in approximately 80% of patients undergoing cTACE and 50% of those treated with DEB-TACE. Median OS varied across studies ranging from 30-44 months with some larger cohorts reporting survival beyond 5 years, with a 5 year OS for cTACE reporting between 28-36%. Tumor response assessed by mRECIST correlates with longer OS (80.5 months in responders vs 39.4 months in non-responders). Patients with pancreatic NET metastases have shorter OS (27.6 months) compared to non-pancreatic NETs (55 months), while PFS remains similar. Poor prognostic factors include extrahepatic disease, liver tumor burden ≥70%, impaired hepatic function, and elevated neutrophil-to-lymphocyte ratios. While cTACE may offer better symptom relief and OS in carcinoid syndrome, DEB-TACE is favored in patients with poor liver function due to fewer post-embolization effects. Although the recent RETNET trial raised safety concerns for DEB-TACE, recent studies suggest a tolerable safety profile. TACE and TAE demonstrate similar outcomes for OS, PFS, and symptom control.
Conclusions: TACE remains a cornerstone therapy for NELM, with strong evidence for symptom control and prolonged survival. While cTACE is often preferred, DEB-TACE may still hold value for select patients, particularly those with compromised liver function, as emerging data challenges prior safety concerns. Direct comparisons between TAE and TACE are limited, but current evidence suggests similar efficacy, warranting individualized treatment selection based on patient comorbidities, liver function, and tumor characteristics.